
 Sorry to start your week out with such a sad story, but I think it needs to be told. Late last week I became aware of the story of Claudialee, a six-year-old girl who passed away after being misdiagnosed with type 2 diabetes, when she actually had type 1 diabetes. There is a very detailed account of the story here.
Sorry to start your week out with such a sad story, but I think it needs to be told. Late last week I became aware of the story of Claudialee, a six-year-old girl who passed away after being misdiagnosed with type 2 diabetes, when she actually had type 1 diabetes. There is a very detailed account of the story here.
I’m not going to go into every detail of this story, but I did want to point out a few things that stand out for me. One is that Claudialee has a family history of diabetes. Another is that the doctor diagnosed Claudialee as obese. It is clear that the doctor was deeply concerned about the young child’s weight–prescribing diet and exercise in an effort to get her to lose weight. It is also clear that the mother closely followed the doctor’s recommendations–carefully monitoring what Claudialee ate and making sure she got plenty of exercise.

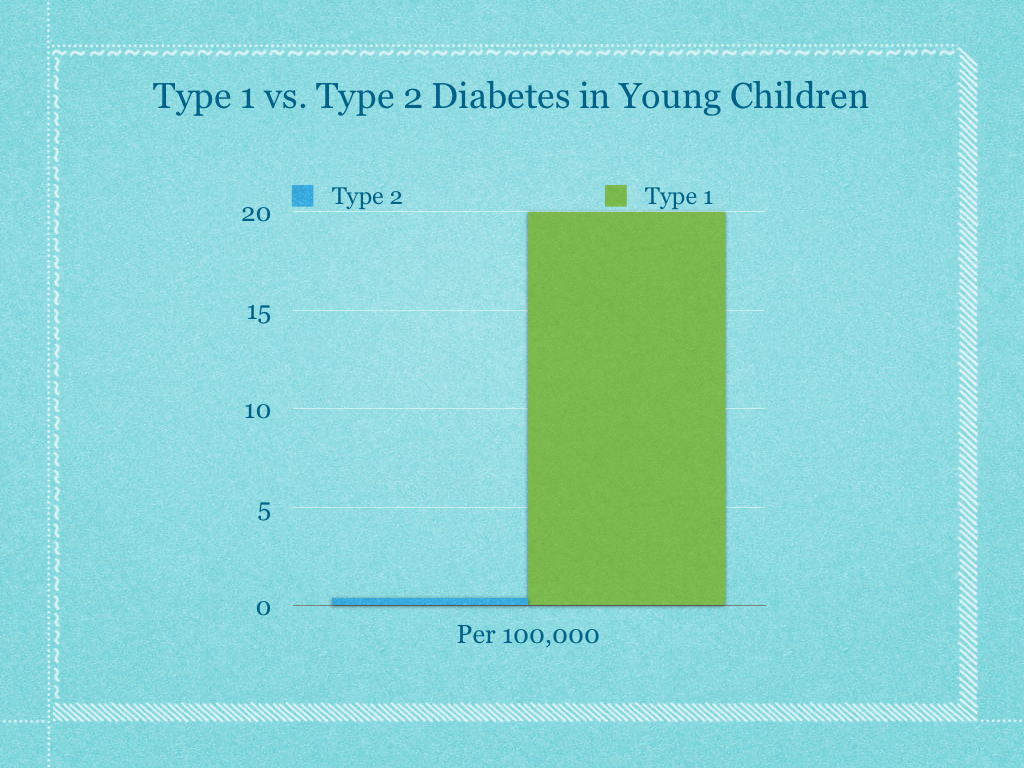
What is not clear is why the doctor felt so strongly that this child had Type 2 Diabetes as opposed to Type 1. According to a source cited in the article (The National Institute of Health) at that age group, Type 1 Diabetes has an incidence of about 20 in every 100,000 kids, whereas Type 2 Diabetes has an incidence of .4 in every 100,000 kids or 1 in every 250,000 kids. What’s more, at that age, Type 1 Diabetes is a far more urgent problem than Type 2 Diabetes. So what led to the doctor’s misdiagnosis?
We may never know for sure. But it does invite one to speculate whether the child’s weight was a factor. Clearly, getting Claudialee’s weight down was a prime part of the prescription to the parent. And as the child’s weight went down, the doctor neglected to do some of the critical follow-up blood tests that would have indicated that something was drastically wrong.
The article states:
Because Mercado [the doctor] had locked in on type 2, she did not monitor her patient’s blood. She did not tell Irma [the child’s mother] to purchase a $20 blood sugar meter from the drugstore. She did not ask Irma about the frequency with which her daughter drank and urinated. And neither she nor Cabatic [another doctor] described to Irma the danger signs to look out for.
When asked in court, why the doctor seemed so certain that the child had type 2 diabetes when type 1 diabetes was so much more prevalent among children that age, she stood by her original diagnosis:
“How many type 2 infant diabetics have you treated?” a lawyer asked her.
“A lot,” she replied. “Maybe it’s geographical, because I work at Brooklyn as an assistant professor and also in wellness program where there are a lot of obese children, so we diagnose a lot of children with type 2 diabetes.”
Clearly there may have been other issues at play here. Claudialee was on Medicaid and doctors are paid significantly less for treating patients on Medicaid than they are for those with private insurance. The doctor was not board-certified, and the article points out that finding board certified physicians willing to work in clinics that take Medicaid can be difficult. And this is a single case where a single doctor has been convicted of malpractice. We will never know exactly what was in the doctor’s mind.
I but I personally found myself wondering if this doctor had ever previously considered that she may have a bias against fat patients–and maybe even fat children with low SES in particular. I wonder, had this doctor considered the potential for her own bias in this arena, would that child still be alive? Would Claudialee still be running around and playing today?
We certainly have plenty of evidence for a seeming “hysteria” around the issue of childhood Type 2 diabetes. A simple google search of “childhood diabetes epidemic” yields hundreds and hundreds of articles. This hysteria has spawned a number of shaming techniques aimed at children despite the fact that shame has been proven over and over again to be ineffective at treating obesity at any age, that shame is more likely to make kids engage in unhealthy behaviors, and that eating disorders are much, MUCH more prevalent among children than diabetes of any kind.
 All I know for sure, is that stories like that of Claudialee get me even more fired up to fight against weight stigma in medicine. And that passion leads me to come to you with a plea. The Association for Size Diversity And Health and the Size Diversity Task force have embarked on a documentary film project to help doctors see and understand weight stigma and weight bias in medicine. This project is called the Resolved project. But this project needs a little bit of help from you. We are raising funds to finish the documentary on Go Fund Me here. Any help you can offer would be greatly appreciated. Even if you can only give a few dollars, that will help. And if you don’t have a few dollars to spend, would you consider sharing this with your friends and asking them to help? Let’s see if we can end weight stigma and weight bias in the healthcare industry for good. And maybe, just maybe we won’t have stories like Claudialee’s any more.
All I know for sure, is that stories like that of Claudialee get me even more fired up to fight against weight stigma in medicine. And that passion leads me to come to you with a plea. The Association for Size Diversity And Health and the Size Diversity Task force have embarked on a documentary film project to help doctors see and understand weight stigma and weight bias in medicine. This project is called the Resolved project. But this project needs a little bit of help from you. We are raising funds to finish the documentary on Go Fund Me here. Any help you can offer would be greatly appreciated. Even if you can only give a few dollars, that will help. And if you don’t have a few dollars to spend, would you consider sharing this with your friends and asking them to help? Let’s see if we can end weight stigma and weight bias in the healthcare industry for good. And maybe, just maybe we won’t have stories like Claudialee’s any more.
Love,
Jeanette (The Fat Chick)
P.S. Want to stay up to date on my projects and appearances? Just opt in RIGHT HERE!


